The Greater Manchester Cancer Alliance is committed to;
- Technical delivery of a remote digital monitoring system for PSFU across Greater Manchester
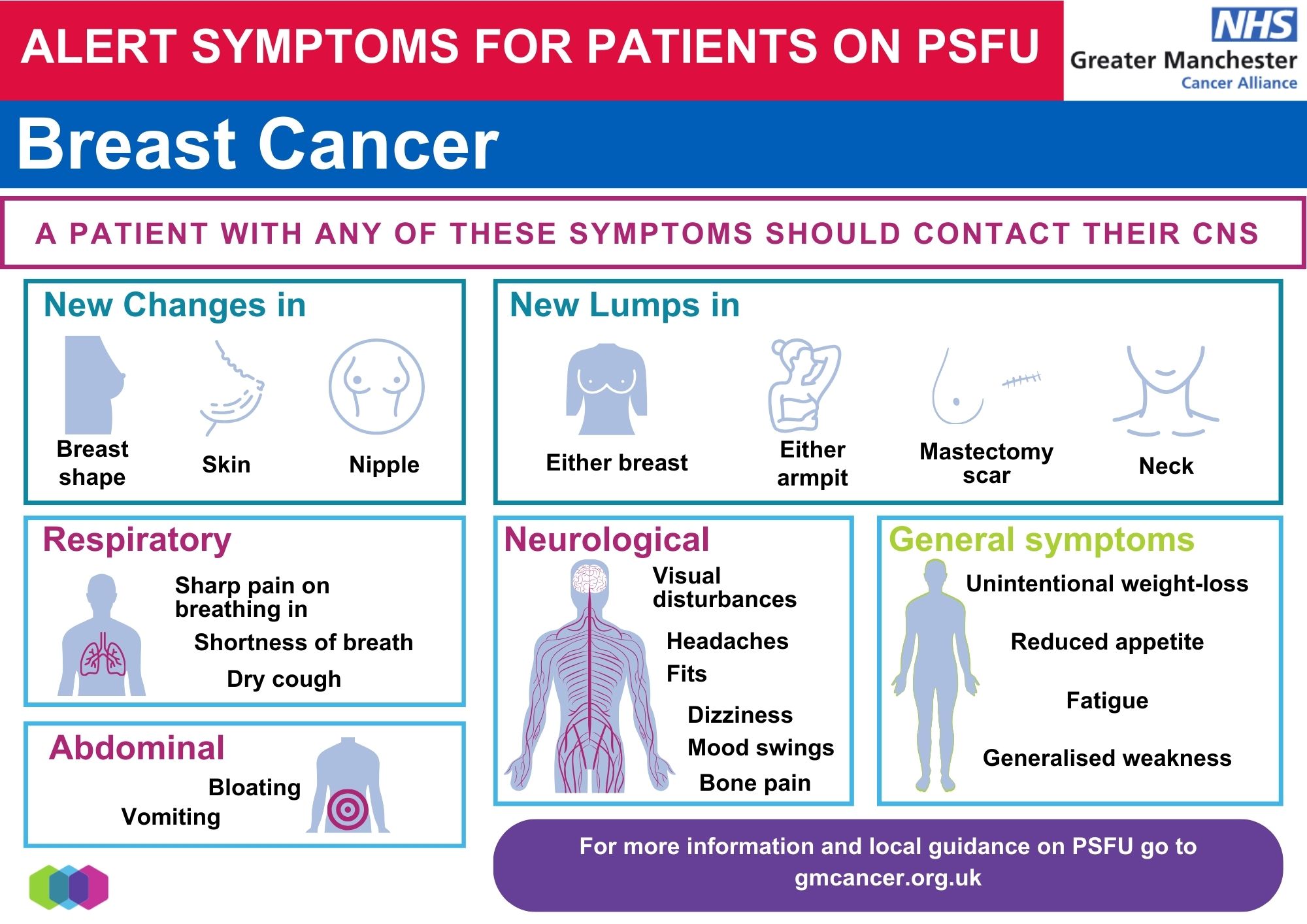
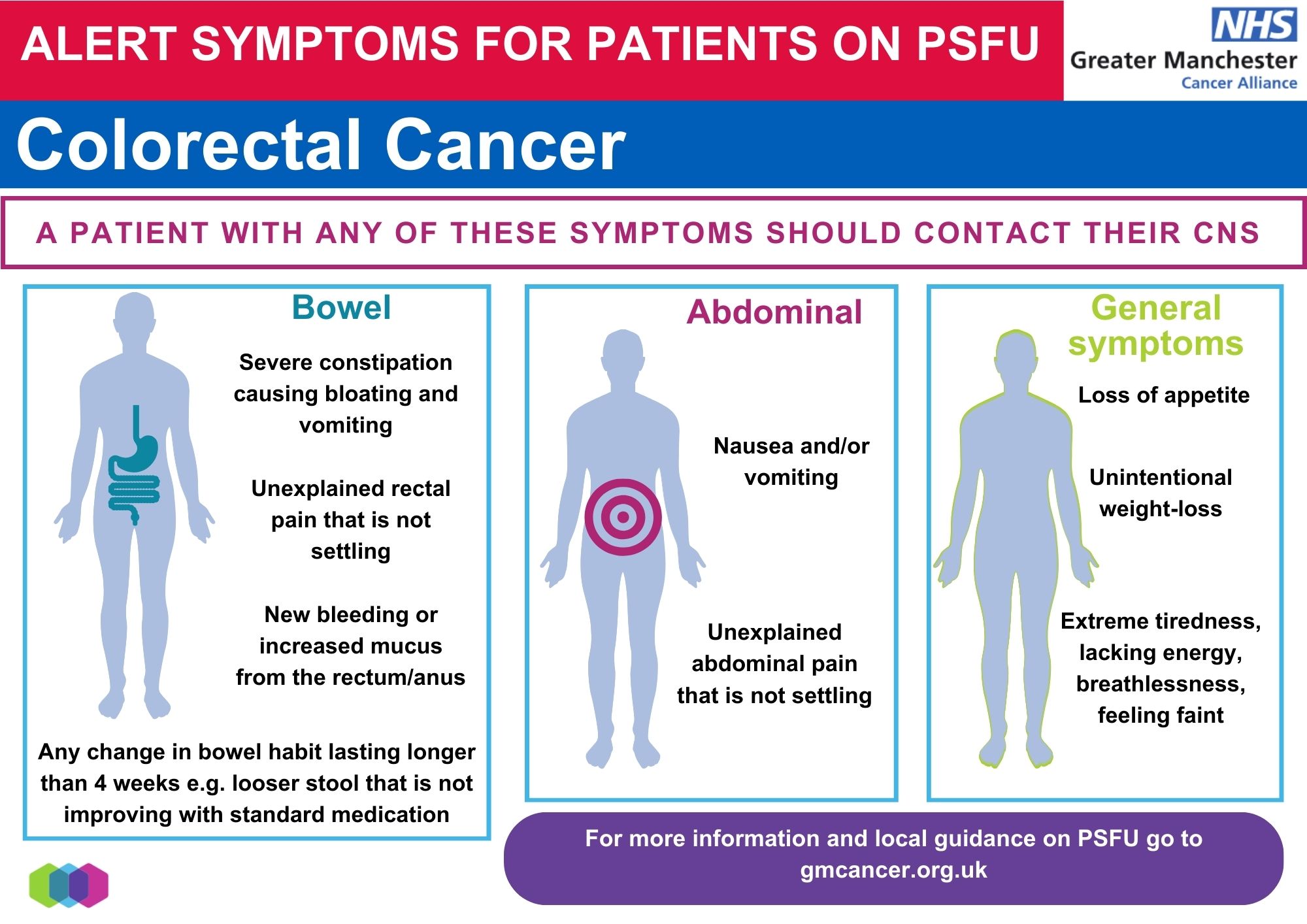
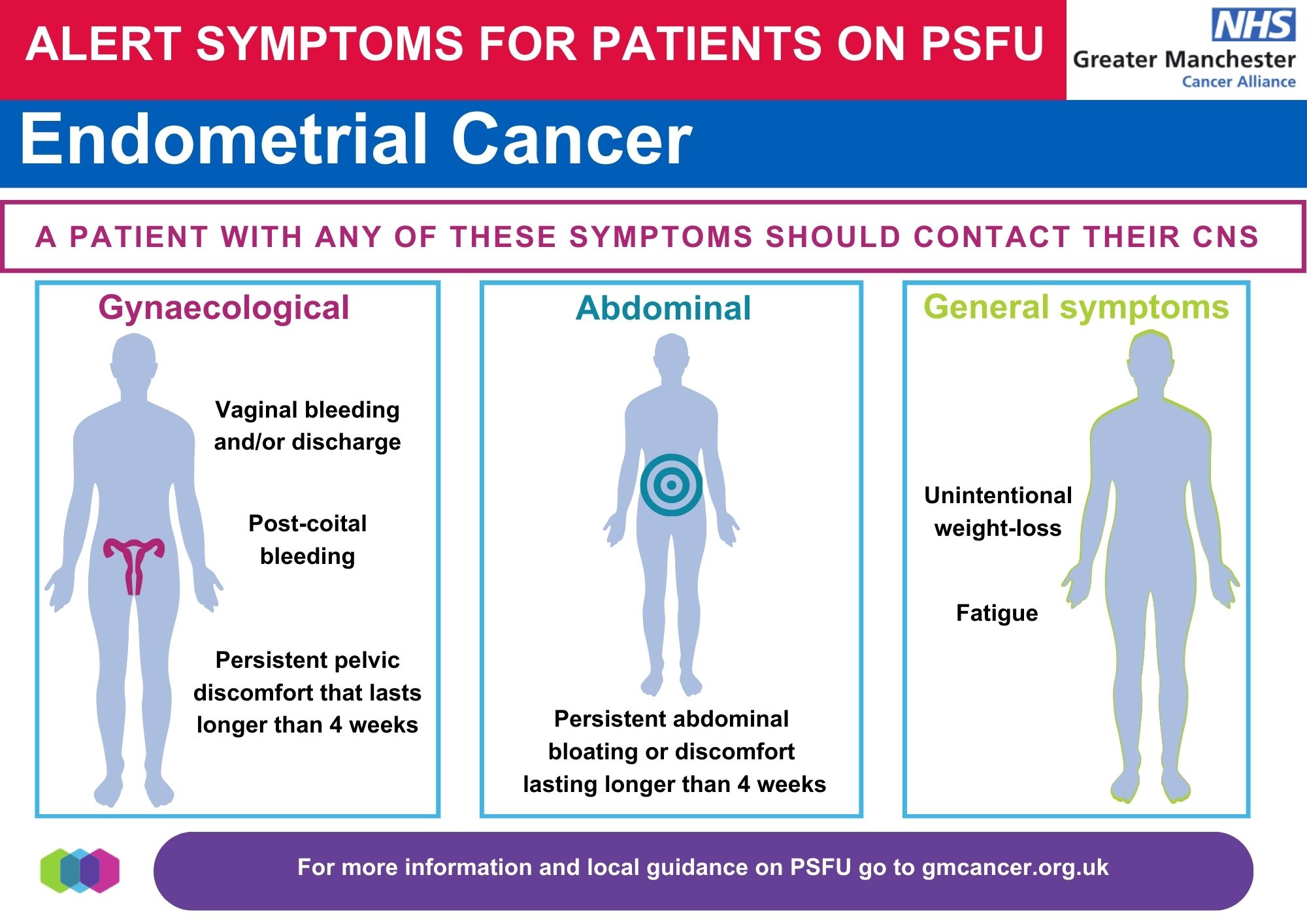
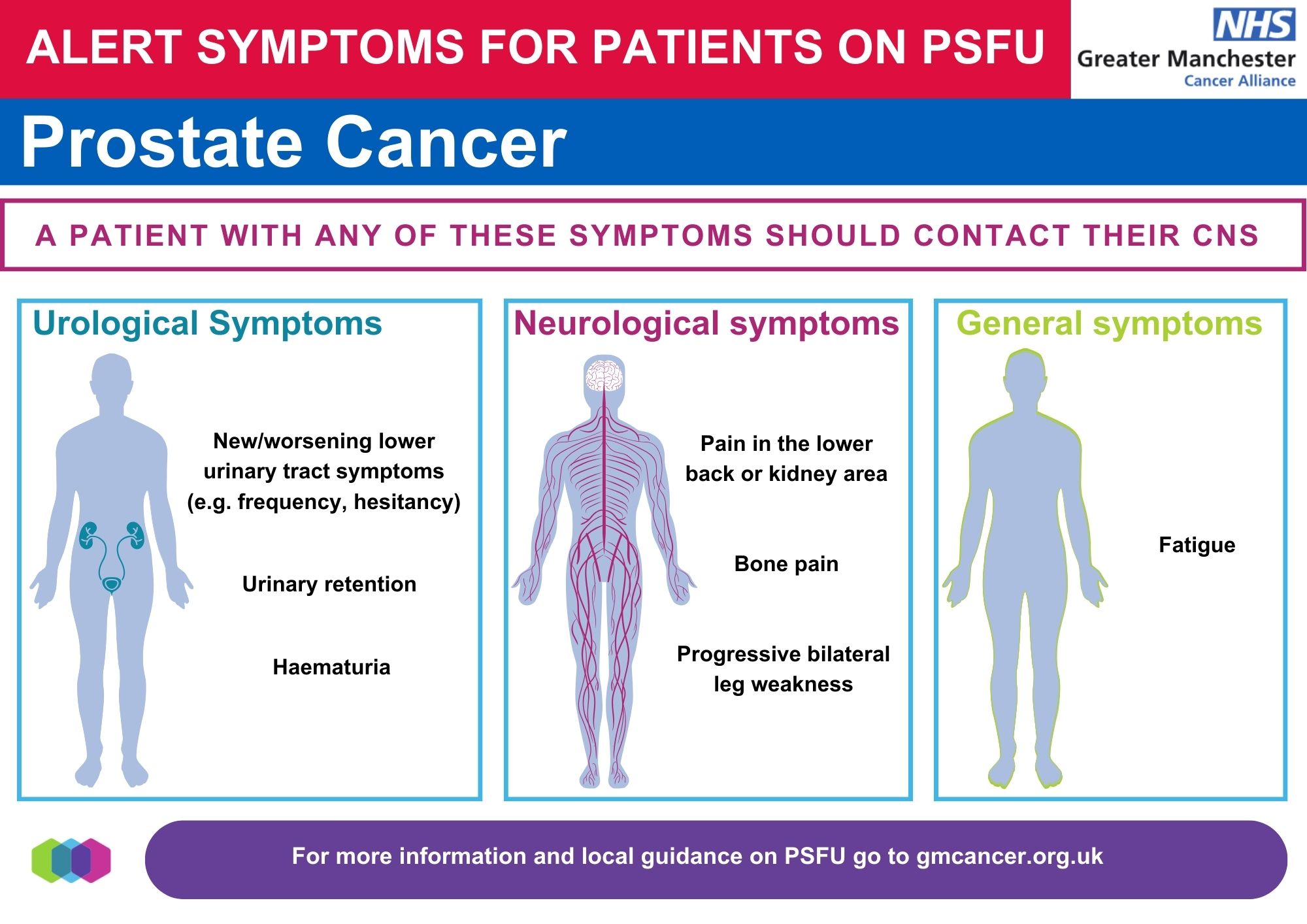
and; - Creating fully operational and sustainable PSFU pathways for all suitable patients in breast, prostate, colorectal and endometrial cancer.
The NHS Operational and Planning Guidance places requirements on Cancer Alliances to support trusts to operationalise personalised stratified follow up pathways for breast, colorectal, gynaecological and prostate pathways.
Patients will be stratified for follow up by their clinician and/or MDT team once active treatment has been completed based on clinical need. Follow up will take the form of professional led follow up (traditional consultant led clinics in an outpatient setting) for those with a higher risk of disease recurrence or self-management for lower risk patients who following treatment will no longer have routine consultant led appointments.
PSFU pathways will include the following key features
- Effective needs assessment at end of treatment that identifies and addresses any outstanding needs and ensures the patient has knowledge and confidence to manage their own care.
- A schedule of follow-up investigations for each pathway which is agreed by the Pathway Board for that tumour group
- Removal of routine follow up appointments from the pathway. The results of investigations will be reviewed by an appropriately qualified staff member and the patient is informed of the results (in line with clinical judgement and local protocols).
- Good communication between specialist, community, and primary care teams.
- A robust digital monitoring system to manage on-going surveillance tests and ensure no-one is missed for follow up tests.
- A system that allows rapid re-entry into the specialist cancer service if required. This reassures individuals that they can access appropriate, named support quickly should they need it without having to go via their GP.
As each PSFU pathway will follow a protocol signed off by the Pathway Board relevant to that tumour group, there will be equity of care across Greater Manchester as every patient follows the same schedule of tests (where clinically appropriate).
Each protocol will also include inclusion and exclusion criteria.
GM Cancer alliance have also written an Equality Impact Assessment (EIA) to ensure that PSFU does not make health inequalities worse. Trusts will also write an EIA which reflects their specific population.
The Benefits of Personalised Stratified Follow Up (PSFU)
For Patients
Access to higher quality care that:
- is personalised and tailored to people’s specific needs and conditions
- is based on what matters to people and their individual strengths, needs and preferences
- helps to detect and manage cancer-related psychosocial problems
- provides more support for those with complex needs
- helps people find services that meet their individual needs, and
- increases the proportion of people continuing to have surveillance tests (ie fewer “lost to follow up”)
Support for self management that:
- provides information enabling earlier self detection of recurrence, progression or long term side effects
- encourages people to contact their healthcare team at any time with worries or concerns
- increases people’s knowledge and understanding of their condition and situation
- increases people’s overall confidence, health and wellbeing, and
- encourages lifestyle changes which can help to reduce the risk / impact of cancer recurrence (or nw cancers), treatment consequeinces and comorbidities
Improves patient experience by:
- reducing travel to hospital (if on remote monitoring)
- reducing anxiety through more timely access to results
For Professionals
- enhanced continuity of care
- better triage of queries by support staff
- more responsive access to specialist teams if problems occur
- improved communication and links with primary care teams (eg via End of Treatment Summaries)
- improved knowledge of management of acute and long term side effects, and
- improved knowledge of pathways for referral / signposting to services and third sector support.
For Systems
- improves productivity through the redeployment of professionals time, outpatient capacity* and reduced duplication of surveillance tests
- supports greater integration of care
- supports better communication across different care settings
- reduces demand for unplanned care, and
- increases the transparency around costs of cancer follow up, allowing resources to be targeted at patients with complex needs.
- modelling suggests that for every 1,000 referrals per cancer type, PSFU could allow redeployment of outpatient slots over the subsequent five years in Breast: 2,850; Colorectal: 2,750 and Prostate: 1,900

{kind=link}
{kind=link}
{kind=link}
{kind=link}